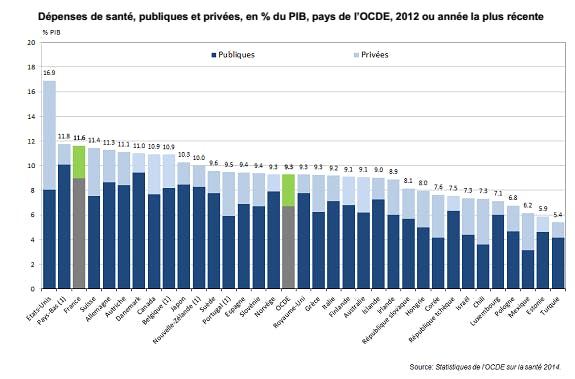
For a long time we thought that our French system was the best in the world. And it was. But, it’s been years that we have observed an increase in costs in our healthcare system, for individuals, while the user experience has not really changed or improved ( worldwide, ranking us #11 in Europe). healthcare Bloomberg ranking France #8 Europe Health Consumer Index Figures are alarming: in France, (yet, it’s below the 18%-level in the US), €250bn every year, and it has been in constant augmentation for the last 50 years. This growth comes with an even larger for our beloved Sécurité Sociale. 11.6% of our GDP goes to healthcare budget deficit And while costs are increasing, satisfaction towards the system is decreasing for every stakeholder including doctors, hospitals, patients… Where does that come from and what can we do? Difference between user and patient First things first, we, the people, are not to be considered as patients anymore. We are users of our . Users when we are patients, users when we assess our risks, but also users when we are healthy. healthcare Semantically, patients are considered an object on which doctors identify symptoms that need to be treated. On the other hand, the user is an active player of his healthcare: he is increasingly the center of attention. The needle will move from physicians monitoring health indicators from time to time to ourselves collecting them in order to share the proper summaries to experts. Indeed, today we are only monitored when something goes wrong, a comparative should analyse “healthy vs. not healthy” and the continuity in-between. medicine Apple Watch Health (source: Hello Heart) We live a crucial moment for this user “empowerment”: (Apple is hiring tons of health experts), by Google, … We will be able to follow our biometrics and our health evolution. In parallel, patient communities are created ( , ) around their diseases. The p̷a̷t̷i̷e̷n̷t̷ user, is the new actor of his health. Apple Watch blood monitoring weight analysis SmartPatients PatientsLikeMe Medicine digitisation The excellent book from Robert Wachter: The Digital Doctor This new healthcare user needs tools to work with his ecosystem of doctors, hospitals, private clinics, insurances… Here comes medicine digitalisation, which has been a slow, painful trend over the last years. This digitising phase took place recently particularly in the US and the UK, with the introduction of the Electronic Health Record (EHR). All information about a patient is supposed to be gathered at one point. If today , hospitals still do not communicate with one another, , and user interfaces are still very poor. Few doctors consider this transition as a success. Mainly, because they have been designed for the ones paying: hospitals who want to optimize their billing and who have beenheavily incentivized by the government to invest in EHRs. more than 70% of American hospitals have an EHR doctors still do not agree on what level of information they should share with patients Dossier Médical Personnel In France, the “Dossier Médical Personnel”, our equivalent of EHR, has been promoted by the government with over . And we haven’t seen any proper private initiatives yet. €500m investment for less than 400.000 subscribers. It has turned into a fiasco What should we see in an EHR? On a user-based approach, I believe it should be the combination of our medical interactions with the healthcare system (doctors you’ve seen and when, which drugs have been prescribed, what have been the diagnoses, lab results, etc…) combined with standard information from wearables and sensors that monitor our health. Google ontact lens to measure glucose in tears. (Credit: New York Times, Google, via Agence France-Presse — Getty Images) Connected devices (wearables, quantified self apps, sensors…) are huge collectors of health data and information. Google is right now working on several sensors to monitor pulse, , with its new brand (formerly Google Life Sciences)… A lot of start-ups such as with its HealthPatch, continuous blood pressure monitoring for , and are very active. Nevertheless, these data will be almost worthless for the end-user if we do not edit the right data-management to analyse information. , and the next big step is to switch from displaying data to generating valuable insight from data. sugar levels Verily Vital Connect Quanttus clinical trials some others Quantified-self does not mean qualified-self Alphabet introducing Verily their new branding for Google Life Sciences We have to move forward a complete EHR system step by step. It does not have to be fully complete and universal from scratch. It is a matter of daily implementation. Doctors tasks will be replaced or completed With this huge amount of information coming from everywhere, the development of new technologies, doctors’ job is to evolve along with the interaction with users. And we hope for the best. I really believe that doctors will remain at the center of our healthcare system for a long time. It is their scope and the way they will be assisted that will change. Da Vinci robotic surgery in action Robotics has started to enter in healthcare mainly with system developed by Intuitive Surgical, that has performed more than 3 million surgeries worldwide. It is still expensive as an investment, every operation requires the purchase of another specific pack, but there is a trend towards more and more robotisation and tools to assist surgeries. Here in France, we have which has not reached the same market penetration yet.New generation of surgery robots is under development with the objective to be autonomous, and to conduct routine surgeries in less time, with less human errors, and ultimately cheaper than standard ones. Will surgery become a commodity accessible to everybody? The question is still open and requires a lot of development. Da Vinci robotic Robot Rosa from Medtech If we can help the hand, we can also help the brain. I spoke in a about Artificial Intelligence (and the difficulty to define it), but we see a trend in machine-learning / artificial intelligence to help doctors take better decisions. is somehow trying to lead the way with the Watson tools. The aim is to distribute them to every single hospital. They have signed deals with (work on rare pediatric diseases), (prediction of health deterioration), Medtronic, or (understanding scientific papers and create a health coach), (providing access to data from apps) in order to support doctors in their decisions on diagnoses and treatments. Deep learning has also proven very useful in image recognition, with companies such as which raised another . previous article IBM Watson Boston Children’s Hospital CVS Health Johnson & Johnson Apple Enlitic $10m for radiology image recognition I believe that AI will enable better diagnosis and personalized medical recommendations, help to scale information and distribute it. It will be the support tool for the new doctors to access, manage and treat data. It follows the same trend that consumer knowledge which has switched from memory to Google. Personalised medicine & prevention This evolution and the huge amont of data we are able to analyse are to be completed by new data-streams and more focus on prevention and healthcare personalisation. Among this, DNA sequencing and analysis is a fascinating topic. The history of genome sequencing is fantastic, beginning with a between public and private initiatives (aka ) to sequence in 2001 the first complete human genome. And since then, cost and speed have improved three times faster than Moore’s law. $100m in 2001 to c.$1,000 today. Not so bad. race Craig Venter Evolution of DNA sequencing costs from $100m to less than $1,000 in 15 years (source: National Human Genome Research Institute) Several initiatives are around to understand better our genome. Not in France of course. National initiatives: UK project with the NHS support, whole country sequencing in , the US and Obama pushing for a with the “Precision Medicine Initiative”, . But also private initiatives such as (Craig Venter again), which mission is to accumulate the largest genomics data set ever with 1 million full human genomes, microbiomes, … 100,000 genomes Iceland $215m sequencing project China announcing even larger numbers Human Longevity Inc. Ling Min Jian; lab technician at the Beijing Genomics Institute (BGI), the world’s largest genome sequencing center. Collecting enormous amount of data is a great challenge that we are addressing now worldwide. But understanding or generating insight from it is even harder. It is like trying to find a bug in a program by looking at the 0s and 1s. You have to get really good eyes and computer power. That’s also why it’s one of the big topic of interest for the GAFA. The excellent of , founder of health website Doctissimo and DNA sequencing DNAVision, are a great read on the topic. articles Laurent Alexandre Illumina’s gene sequencer (Credit: Illumina) Nevertheless, sequencing is changing specific parts of personalised medicine. The one I want to focus on is cancer sequencing. By sequencing blood samples, we detect cancer earlier, we can select and test treatments based on your cancer genetics, and thus we can dramatically reduce costs and risks. Two companies recently raised $100m each in the field: and through Bill Gates, Jeff Bezos, and . Of course, we are still at the beginning and industrial scaling will raise new questions, but it’s out there. Guardant Health GRAIL initiative Illumina Once we can analyse your genome, microbiome, environmental interaction we could be able to target treatments, anticipate diseases… We already see that machine-learning analysis of demographics and somehow epigenetics data (in the broad sense) gives us great assessment of individual risks in order to be guided in the healthcare system. I see two steps in the progress: first a better understanding of our risks to develop diseases based on an overall appreciation of who we are and that will leads us to meet the right doctors at the right time. My hope is that soon enough these doctors will have the best tools to personalise the way they help us to be healthy. All these technologies, for what? Towards new players to serve users As I said before, we are now to be considered as users. And as users, we take informed decisions on what we should buy. One of the central players in the healthcare system is health insurance and sadly, health insurance is one of the last industries which has done nothing to make things accessible: we don’t know what we pay for, what the level of service is, if there is any service at all... In the US, statistics say that . This market status in the US is well documented in this . Metrics seems to be similar in France even if less documented. only one out of seven Americans understands the basic components of a health-insurance plan (Journal of Health Economics) great series of articles The complexity arises from several factors: a multi-stakeholder market (I am not the one choosing how I treat my symptoms, it is the doctor who makes the choice), a complex billing process (shared between doctor, Sécurité Sociale, Complémentaire Santé, reste à charge, ticket modérateur…), no user-centric focus. Indeed, even if you wanted to interact more with your health insurance, the user experience would be really poor today. We don’t understand benefits, websites are far away from what we see in other fields, and it looks like an insurer’s objective to make his customer service difficult to reach. It obviously creates strange dynamics and misalignment of interests. The interactions with your insurance are just about transaction, confrontation . “how can I get paid back as fast as possible?” Nevertheless, I believe that we are today at the edge of a new beginning where product design and technologies can help us to create a user-centric insurance where everything is about giving the best experience. In the US, some start-ups with very interesting metrics of adoption have paved the way: in New York, or . Oscar Collective Health Clover Health In France, we can improve the understanding of what we pay for, how we can navigate in this complex and sometime unfriendly healthcare system. It means building trust between players (the patient, the doctor, the insurer) and going towards more active and personalized prevention. A great health insurance should help us do that. It should be the platform to reach all the technologies and services we have started to analyse in this article, always thinking of what is best for its users. It is a dramatic switch from what exists today, but it can be done with the right focus and technologies.